Summary
...
| width | 70% |
|---|
The Cancer Imaging Program of the National Cancer Institute (NCI) in collaboration with the International Society for Biomedical Imaging (ISBI)
...
have launched a grand challenge in
...
the prostate gland based on magnetic resonance imaging (MRI) data. The challenge will take place at the ISBI Symposium
...
, April 7-11, 2013 in San Francisco, CA.
...
Healthcare Context
...
Recently, the high spatial resolution and soft-tissue contrast offered by MRI makes it the most accurate method available for obtaining this kind of information. This, combined with the potential of MRI to localize and grade prostate cancer, has led to a rapid increase in its adoption and increasing research interest in its use for this application. Furthermore, the medical image analysis and clinical community has been very interested in developing accurate prostate MRI segmentation methods which apart from accurate, automated prostate volume segmentation also serve an important purpose for computer-aided detection and diagnostic algorithms, as well as a number of multi-modality image registration algorithms, which aim to enable MRI-derived information on anatomy and tumour location and extent to aid therapy planning and guidance.
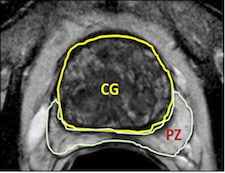
The prostate gland consists of internal structures including the peripheral zone (PZ), central zone (CZ), and transition zone (TZ), where the latter 2 structures are jointly referred to as the central gland (CG). While most tumors are found in the PZ, tumors can also be found in the CG, and CG tumors can have drastically different appearance than PZ tumors. In the PZ (where most cancers are found), tumors are typically chacterized by hypointense regions on MRI images, in stark contrast to the usually hyperintense PZ regions. However, in the CG, tumors are typically noticeable due to their homogeneous texture, as compared to the traditionally hetergeneous texture in the CG. In recent years, several computer aided detection (CAD) systems have been developed for detecting tumors from prostate MRI imagery. Since the tumors in the PZ can appear drastically different from tumors in the CT, CAD systems would invariably benefit from knowing where each internal prostate structure was located.
...
Prostate cancer is the second most common cause of cancer deaths in males and will inevitably afflict 1 on 6 during their lifetime. Difficulty in properly defining prostate anatomy lies at the heart of a problem in which many diagnostic prostate biopsies fail to detect the presence of occult cancers. Approximately 20% of ultrasound image guided prostate biopsies return negative results despite rising blood levels of PSA marker and presence of cancer somewhere in the 30+ cc gland. These failures have been attributed by some to the hesitation to sample one of the two major zones of the gland - namely the predilection toward the more easily reached "peripheral zone (PZ)" over the less accessible "central zone (CZ)". This year ISBI challenges contestants to outline these two non-overlapping adjacent regions of the gland.
Advancing solutions to this vexing clinical problem will surely gain recognition of the power of computer image processing to address a widespread but critical healthcare puzzle.
...
Open and closed source algorithms applicable to both 1.5T and 3T MR images will be most welcome
...

...
.
...
Challenge Structure and Time Line
Data for the prostate challenge has have been provided by Boston University and Radboud University, Nijmegen Medical Centre (the Netherlands). The challenge data has been , divided into three groups:
- January 26: Training cases have been will be made publicly available to all interested participants. This consists of 60 subjects, half of which taken from the Prostate-Diagnosis collection (1.5T) and the other half from the Prostate-3T collection (3T). Ground truth Reference Standard (or Ground Truth) data for each subject will also be are provided in the form of NRRD image segmentations created by expert observers.
- March 7: Leader Board cases will be made available closer to the date a month ahead of the conferenceNCI-ISBI Challenge. Participants in the contest will be able to submit their segmentation results for evaluation using this data set. This will consist of 5 additional 10 cases from both the Prostate-Diagnosis collection (1.5T) and the Prostate-3T collection (3T). NRRD segmentations used for generating participant scores will be held by the contest organizers.
- March 7: Prospective participants for the Onsite Challenge Test must submit a 1-page abstract to include title, authors, affiliation, objectives, data, methods, results and conclusions. Format: 11 point font, PDF.
- April 7: The 2013 NCI-ISBI Grand Challenges Challenge will be held on the last day of the conference (Thursday, April 11th)at the ISBI annual meeting in San Francisco, CA. Testing data will be made available to participants at this time, which will again consist of 5 additional 10 cases from both the Prostate-Diagnosis collection (1.5T) and the Prostate-3T collection (3T).
...
A 60 case prostate MRI 3D series "training set" consisting of DICOM images with matched .NRRD markups that defines the tissue "central zone (CZ)" and "peripheral zone (PZ)" are available from the National Cancer Institute (NCI) via The Cancer Imaging Archive – "TCIA".
...
There will be 60 cases, each consisting of 15+ (4 mm thick slices at 3T) or 28+ (3 mm thick at 1.5T) adjacent axial cross-section cuts. Half of them were obtained at 1.5 T (Philips Achieva) with an endo-rectal receiver coil (from (BMC) Boston Medical Center) and the other half at 3T (Siemens TIM) with a surface coil (from from Radboud University Nijmegen Medical Centre (RUNMC), Netherlands). They were acquired as T2 weighted MR axial pulse sequence. Each file contains nearly all DICOM acquisition parameters except tags that specifically identify Private Health Information (PHI).
...
- Prostate-Diagnosis Segmentations (coming soon)
- Prostate-3T Segmentations (coming soon)Segmentations
Submitting Your Results
Once you've trained your algorithm on those 60 cases the NCI-ISBI Challenge Committee will provide you access to a new 10 case "LeaderboardLeader board" set to which you will not have .NRRD markup data. "LeaderboardLeader board" is a popular term (borrowed from golf) for a procedure to see how well you are doing on a pre-test set to get a sense your relative competitive rank before submitting to a final test. The results of your participation in the Leaderboard Leader board will be returned to you as feedback on a subset of sequestered markups retained on the judging analytic software using Kitware's MIDAS software. You may then use those results for further tuning your algorithm to prepare yourself for the final "Test" set of 10 totally new cases on which you will run your algorithm while attending the ISBI meeting in April 2013.
...
| Section | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|